By Andrew Sorfleet
How do you determine who is at high risk for HIV infection?
According to Health Canada’s July 2016 safety brief on Truvada for HIV pre-exposure prophylaxis, “exchange of sex for commodities (e.g. money, food, shelter, drugs)” is a factor that “may help identify a person at high risk of HIV infection.”1
In October 2016, funded by a grant from Elton John AIDS Foundation, Triple-X in partnership with the Dalla Lana School of Public Health, University of Toronto, organized and hosted a national consultation and invited 23 organizations from 10 provinces and territories who provide advocacy or services for sex workers.
Fifty women, men and trans people from across Canada that work with sex workers met in Toronto. The purpose of this national consultation was to give participants the opportunity to educate themselves, explore and grapple as a group with the implications of PrEP on the sex industry. PrEP (HIV pre-exposure prophylaxis) is the idea that a person could take a pill once a day and be protected from catching HIV, not unlike the birth-control pill which protects from unwanted pregnancy.
The “PrEP in the Context of Sex Work” meeting was held in response to the intention to make PrEP accessible to sex workers, because sex workers are considered at high risk for HIV infection. But, where did this idea come from?
Safe Sex Professionals
For 30 years now, sex worker activists have stated that: “Prostitutes are Safe Sex Professionals.” Sex workers are best placed in society to provide hands-on HIV prevention education and demonstration, with the very large and invisible portion of the public who are clients. What is annoying about this “key population” approach is that sex workers are not given any professional respect by HIV research that targets prostitution. It ignores the fact that sex workers should be a priority for HIV and STI prevention education and funding, not because sex work is a risk factor for HIV transmission, but because, to quote Valerie Scott in 1989:

“Whores are safe sex pros. We’re the ones who put the condoms on the guys. We’re the ones who do the education. And what do we get for it? At conferences like this all we get is shit on. ‘Prostitutes are spreading AIDS.’ That’s bullshit! As I said the other day, if that were true, half the government would be dead already.”
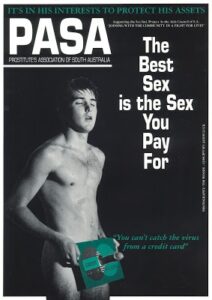
Sex work is most often defined in HIV research to include ambiguous transactions, such as trading sex for commodities, a place to sleep, meals, etc. What can’t be distinguished with this definition is whether perhaps the risks for HIV are poverty and desperation, and not sex work as an occupation at all. Sex workers after all, need to protect their sexual health to be able to work. Like this 1990 education poster from Prostitutes Association of South Australia says:
“It’s in his interests to protect his assets. You can’t catch the virus from a credit card.”
(PASA), c.1990.
Courtesy of Australian Lesbian and Gay Archives
Truvada PrEP Approved
On July 16, 2012, the U.S. Food and Drug Administration announced their approval of Truvada for HIV pre-exposure prophylaxis (PrEP). Truvada was already approved for many years as an HIV treatment medication. Now, it could also be used as a prevention medication. Truvada’s safety and efficacy for PrEP were demonstrated in two large, randomized, double-blind, placebo-controlled clinical trials, according to U.S. FDA press release:
“The iPrEx trial evaluated Truvada in 2,499 HIV-negative men or transgender women who have sex with men and with evidence of high risk behavior for HIV infection, such as inconsistent or no condom use during sex with a partner of positive or unknown HIV status, a high number of sex partners, and exchange of sex for commodities.”2
February 2015, Health Canada approved Truvada for HIV PrEP in Canada. Once approved, regional health authorities and national advocacy groups began drafting guidelines for prescribing Truvada as PrEP, an important step towards having it listed for public access — free for those at high risk of HIV infection, paid for by government.3
“High Risk” = Sex Work Stigma
The B.C. Centre for Excellence in HIV/AIDS research had already released guidelines for Truvada PrEP in 2014:
“Before starting PrEP, confirm that the patient is at ongoing high risk for acquiring HIV infection. …this will usually consist of having one or more of the following.”
Among the list was “involvement in commercial sex work,” and “having sexual partners who are MSM (men who have sex with men) or use injection drugs or who are involved in commercial sex work.”4
In the United States, state governments also released guidelines for prescribing PrEP and assessing high risk of HIV infection. The New York State Department of Health AIDS Institute and the Centers for Disease Control and Prevention for example (Summary Statement on Pre-Exposure Prophylaxis to Prevent HIV Infection, October 2015):
“Providers need to obtain a thorough sexual and drug use history and regularly discuss risk-taking behaviors with their patients to assess candidacy for PrEP, encourage safer-sex practices and safer injection techniques (if applicable), and assist in the decision of when to use PrEP and when to discontinue use.”
In a table labelled “Potential Candidates for PrEP,” “Individuals engaging in transactional sex, such as sex for money, drugs, or housing,” are listed. However, all other candidates such as MSM and IDU (people who inject drugs) must ALSO be engaged in “high-risk behaviour.” This requirement, however is not listed for sex-worker candidates.5
At the 2016 Canadian Association of HIV Researchers (CAHR) conference in Winnipeg, CANPrEP — an ad hoc committee of HIV prevention professionals, doctors and researchers, supported by the Canadian HIV Trials Network funded by the federal government through the Canadian Institutes of Health Research — presented draft guidelines for prescribing Truvada as PrEP. These guidelines also mentioned “sex trade workers” as one of the groups with a “significant risk of having transmissible HIV.”6

at The Forks in Winnipeg for the 2016
annual CAHR conference. Photo: Shawna Ferris
Sex Workers Push Back
During their presentation at CAHR, it became apparent that CANPrEP researchers had failed to consult sex workers when drafting their proposed guidelines. In response to this, delegates from seven organizations from across Canada who work with sex workers drafted an eight-page letter:
“To suggest that sex workers are a population at higher risk for HIV infection and transmission assumes that professional sexual services are not performed safely in an occupational setting. This is a gross generalization. You have provided no evidence or references for this.”
The letter goes on to say:
“To focus guidelines for assessing risk on populations rather than activity is in its own way stigmatizing. To quote the ‘Principles and Beliefs,’ Maggie’s Constitution, Toronto Prostitutes’ Community Service Project, 1993:
“There are no high risk groups, only high risk practices. AIDS and sexually transmitted diseases (STDs) are not spread by sex work; they are spread by unsafe sex and needle sharing.”7
According to the Ontario HIV Treatment Network (OHTN), in a July 2012 brief titled “Sex Worker HIV Risk:”
“Establishing the prevalence of HIV among sex workers is challenging because they are a hard-to-reach population. Estimates range from 1% to 60%.”
Of 11 studies reviewed, only two addressed women working in indoor settings. Four studies assessed street youth specifically (“involved in survival sex”), three included only female drug users, one recruited Aboriginal women. OHTN were involved in developing the CanPreP guidelines. Their Rapid Response brief postulates:
“There are three main categories of risk for HIV infection among commercial sex workers in Canada: high risk sex or sex with high risk partners, illicit drug use, and unstable living and working environments. Other risk factors include young age, tattooing or body piercing, and a history of sexual abuse.”
The OHTN “Sex Worker HIV Risk” brief then states:
“Little is known about these issues in Canada and other high-income countries. In the Canadian context, injection drug use among sex workers and heterosexual transmission to clients and then to their sexual networks is contributing to the HIV epidemic.”8
“High Risk?” Or “Key Population?”
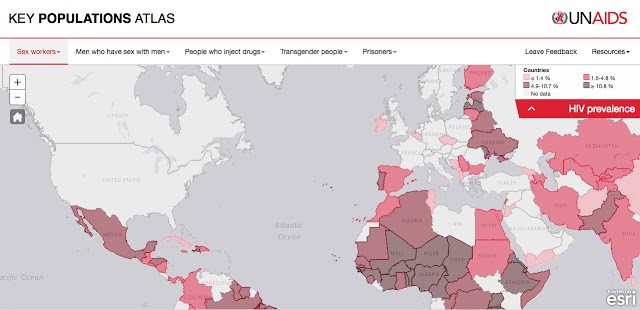
The UNAIDS Key Population Atlas is divided into five categories: Sex Workers, Men Who Have Sex With Men, People Who Inject Drugs, Transgender People, and Prisoners. This website/app gives you UNAIDS statistics on HIV prevalence by country for each “key population.” One of which is “sex workers.” There’s a drop-down menu where you can choose statistics for population size estimate, condom use, knowledge of HIV status, and more. “Condom use” is defined as “Percentage of sex workers reporting the use of condom with their most recent client.”
How intrusive would public health research need to be to collect that data from sex workers?
Currently, this data is mined from pre-existing research and numbers are calculated using meta-analysis software. There is a wealth of data from decades of concentration of HIV research in high HIV prevalence countries such as in sub-Saharan Africa and parts of Asia Pacific. However, in countries where HIV prevalence rates are low, there is little HIV prevalence research on sex workers, which includes knowing the size of the sex-worker population in a given region. And where prostitution is illegal, operating clandestinely, estimating population sizes is challenging.
The UNAIDS Key Population Atlas legend uses grey to indicate “no data.” When you select “sex workers” and “HIV prevalence” you will see there is no data for most of North America, as well as most of Europe and the Middle East.
Lack of Research = Flawed Statistics
In July 2014, in conjunction with the 20th International AIDS Conference held in Melbourne, the Lancet published a special issue on Sex Work and HIV. The second page is an infographic that states that 0.8% of the global general population has HIV. In comparison, 11.8% of female sex workers, 14% of male sex workers, and 27.3% of transgender women sex workers globally have HIV.
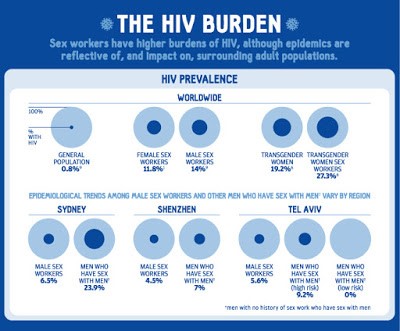
It’s curious how these global statistics were calculated given that there are not even population size estimates for sex workers in almost half of the world. What is also misleading, is that countries where sex workers have a high HIV prevalence rate tend to be countries with a very high rate overall. In a region where HIV is very low, you are much less likely to ever be exposed. Comparing an average rate for sex workers in high HIV prevalence countries to a global average is completely out of context.
“Sex workers are central to African HIV epidemics,” the opening editorial states, “more than 50% of sex workers living with HIV are all in sub-Saharan Africa. 92% of all HIV/AIDS deaths attributed to sex work occur among African women.” The editorial goes on to speculate that:
“With heightened risks of HIV and other sexually transmitted infections, sex workers face substantial barriers in accessing prevention, treatment, and care services. Why? Because of stigma, discrimination, and criminalisation in the societies in which they live. These social, legal, and economic injustices contribute to their high risk of acquiring HIV. Often driven underground by fear, sex workers encounter or face the direct risk of violence and abuse daily. They remain underserved by the global HIV response.”9
Another article in the special issue on HIV and Sex Work titled “Global epidemiology of HIV among female sex workers,” explains more the origins of the global sex worker statistic:
“Worldwide, sex workers are disproportionately affected by the HIV pandemic. … a review of HIV burden in female sex workers (FSWs) in 50 low-income and middle-income countries reported an overall HIV prevalence of 11·8% with a pooled odds of HIV infection of 13·5 compared with the general population of women of reproductive age.
“In many high-income countries and regions, such as Canada, the USA, and Europe, epidemics that initially escalated in people who inject drugs in the mid-1990s shifted to FSWs. In settings such as Russia and central and eastern Europe, the scarce data available suggests emerging or established epidemics among FSWs who inject drugs.”10
These conclusions from that review, published in the Lancet March 2012, were drawn from:
“102 selected articles and surveillance reports from 2007 to 2011 … representing 99,878 female sex workers in 50 countries. In 26 countries with medium and high background HIV prevalence, 30·7% of sex workers were HIV-positive and the odds ratio for infection was 11·6.”11
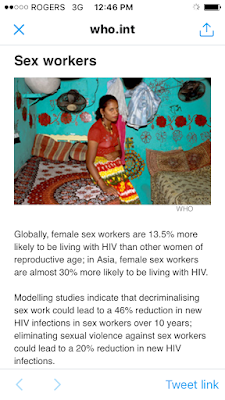
This statistic still has currency today. According to the World Health Organisation webpage on HIV and Sex Workers (January 28, 2018):
“Globally female sex workers are 13.5% more likely to be living with HIV.”
HIV Research? Or Invasion of Privacy?
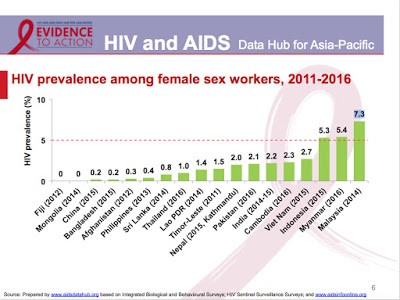
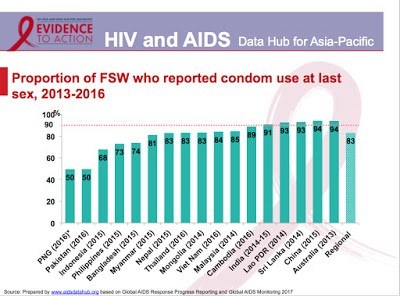
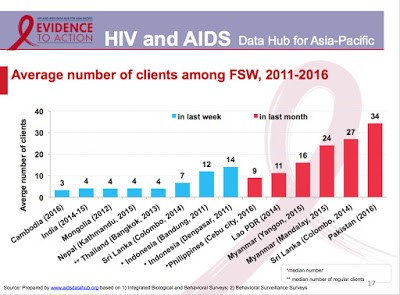
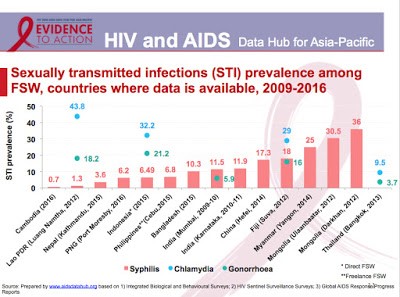
This 2017 slideshow from AIDS Data Hub, “Review in Slides: Female Sex Workers,” shows HIV statistics for sex workers for the WHO global region, Asia-Pacific. UNAIDS statistics includes research data not only on population size estimations and HIV prevalence rates for sex workers but also:
- sexually transmitted infection prevalence
- proportion of FSW who reported condom use at last sex
- proportion of sex workers under 25 years of age
- average duration in the profession of selling sex
- average number of clients (last week, last month)
- proportion of FSW who reported consistent condom use with their clients
- proportion of FSW who inject drugs
- proportion of female sex workers who have been forced to have sex in the last year
- proportion of FSW with comprehensive HIV knowledge.12
Meanwhile in Canada
Canadian Institutes for Health Research (CIHR) and other national and international research foundations will prioritize funds for research that can provide data for UNAIDS Key Population HIV statistics. This data is necessary to measure progress on the 90-90-90 Goal to End AIDS by 2030 (Global AIDS Response Progress and Global AIDS Monitoring). Organizations that provide support services for sex workers will be pressured through funding to participate in research on their clients. These numbers will set priorities for HIV programming in the provinces/territories.
Attempts to gather sex-worker data on HIV prevalence are underway in Canada. In 2015 here in British Columbia, the B.C. Centre for Disease Control (BCCDC) partnered with the Pacific AIDS Network (PAN), the B.C. Centre for Excellence in HIV/AIDS (BCCfE) and other key provincial stakeholders and contracted the Centre for Global Public Health (University of Manitoba) to develop size estimates for priority populations in B.C.:
“It is well understood that a few key populations in British Columbia bear a disproportionately high burden of HIV and hepatitis C compared to the general population. These key populations include gay men and other men who have sex with men (MSM), people who use injection drugs (PWID), and heterosexuals who engage in high-risk behaviours (i.e., sex work).
“In order for HCV and HIV services to determine if their programs are adequately serving these key populations, they need reliable estimates of key population sizes, ideally in their local jurisdiction. However, these estimates are difficult to get because many of these populations are hard to reach or hidden due to stigma, or occur too infrequently to be measured through the usual methods (i.e. censuses).”13
Triple-X was asked to participate in this population estimate project, but we politely declined, stating that involvement in a project with the provincial health authority at this time would undermine our efforts to gain trust and recruit members. Which is absolutely true.
In the final report, this “Cautionary Note” was my contribution, during our correspondence:
“A key informant remarked that ‘counting’ SW may perpetuate the stigma and discrimination faced by SW as being more impacted by HIV than the general population. It was noted that risk for HIV infection is not inherent in sex work. Sex work is different from other social-sexual behaviours, because for the most part, sex work is performed in the context of employment for income generation.”
The section goes on to state:
“In fact, a SW study conducted in Victoria (n=201 adult SW aged ≥ 18 years, including 160 female, 36 male and 5 transgender individuals) has shown that condom use with clients among SW exceeds 90%, indicating that professional sexual services are performed safely in an occupational setting. However, there are individuals engaging in survival sex work or transactional sex in informal settings who may not identify as sex workers. These individuals may be faced with other issues such as poverty, violence (including intimate partner violence) and drug addiction that increase their risk for HIV/HCV acquisition. Therefore, for the purpose of HIV/HCV programming, a clear definition of a priority population based on behaviour and context that impose risk, rather than a general identification with a group, is needed.”
In the following section however, “Supplementary Information on Sex Work as a Potential Risk Factor for HIV Acquisition,” there are sex work statistics gathered by the BCCDC on people who have tested positive for HIV. It states:
“Historically, it has been assumed that sex work plays an important role in the heterosexual and same-sex transmission of HIV. …the project team requested the BCCDC Surveillance Team to perform an analysis on new HIV diagnoses among men and women in BC from 2006-2015 to determine what proportion of these cases reported sex work as a potential risk factor. We found that the number of women diagnosed with HIV and who reported sex work declined from 22 and 26 individuals in 2006 and 2007 to only 2 and 1 individual in 2014 and 2015. Injection drug use was also reported by 33% — 100% of these women over the same period.”14
The BCCDC (the provincial health authority) questions people who test HIV-positive about whether sex work was a risk factor in their infection. The report also notes that 100% of those who reported sex work also reported injection drug use.
#SWPrEP 2016 Report
To report back on the national consultation in Toronto, Triple-X and DLSPH produced a book: #SWPrEP: HIV Pre-Exposure Prophylaxis and Sex Work in Canada 2016. The book was launched at the annual CAHR conference in Montreal, April 4, 2017. The book contains the transcripts of all the presentations, as well as the discussions that ensued between sex workers and those who provide services for sex workers. #SWPrEP participants were clear about some things they wanted to see in the report, and the Facilitator’s Summary (p. 135) highlights the top-ten concerns coming out of the consultation.
Among those concerns, participants did not want PrEP side effects played down. They wanted PrEP to be presented within the spectrum of HIV prevention and for more and equal promotion of condom use. They wanted educational presentations from healthcare professionals as well as from PrEP critics.
Furthermore, sex workers and sex work advocates were concerned that this new HIV prevention drug could result in elevated risks for sex workers, including new pressures from market competition to provide services without condoms if there is an expectation that sex workers should be on PrEP.

In addition, “#SWPrEP,” a seven-minute video that teases out the issues discussed at the consultation was released.
On June 11, 2017, as part of the 5th Annual Red Umbrella March, Triple-X and PACE hosted an afternoon discussion to present the #SWPrEP report and screen the #SWPrEP video for the consultation participants from Vancouver as well as for anyone else who was interested in the topic of sex work and PrEP.
The results of the national consultation were widely well received. By the end of November 2017, the website recorded 51,000 downloads of the #SWPrEP book since the time of its release in March. The Canadian AIDS Treatment Information Exchange (CATIE) reported that “Conversations That Matter — Sex Workers & PrEP” (posted May 16, 2017) was the 8th most read blog post of 2017.
#SWPrEP: Why Does It Matter?
Truvada will not be the only HIV prevention product being sold to governments for people at high risk. There new ARV pills, injectables, and vaginal rings and gels.
There are also HIV vaccines going into clinical trial phase. The drug company Johnson & Johnson has designed a vaccine to treat all strains of HIV, which has already proven to be 100% effective at achieving immunity against the virus after a trial of 350 volunteers.
“For this first large trial, the most at-risk people in the population will receive the vaccination and will include 2,600 young women (18-35 years) from five different African nations.”15

There are also new ultra-sensitive HIV spit-testing technologies being developed for on-the-spot testing. In a research study released January 22, 2018, this new HIV Oral Fluids (OF) Test:
“could be broadly deployed to screen at-risk populations using OF in many settings, including those … where needles are inconvenient (pediatrics) or unsafe (prisons).”16
Such broad deployment could include on-the-spot testing of sex workers in the workplace.
Sex Workers’ Rights are Labour Rights
There is a history of governments and employers trying to force medical treatments on workers in the name of public health and safety. One notable and relevant dispute is here in B.C. between the provincial health authority and the B.C. Nurses Union.
In November 2017, health authorities started to remind members of their obligation to receive the flu vaccine. As per the policy, health care workers must be vaccinated against seasonal influenza or wear a mask at all times during the declared flu season. The policy has been under dispute since it was introduced in 2012. BCNU has always opposed mandatory flu vaccinations:
“Nurses and other healthcare workers should have the right to decide whether to be vaccinated against influenza, based on their understanding of the current evidence and in discussion with their own family physician or other care provider.”17
BCNU filed an industry-wide application dispute (IWAD) last fall that has since been referred to arbitration.
In another recent labour decision in B.C., United Steel Workers (USW) won an arbitration January 29, 2018 that puts an end to random drug testing by Teck Resources at its unionized coal mines in the Elk Valley. Teck began random testing employees in December 2012. The arbitrator completely rejected the idea that some theoretical, but non-existent safety risk justifies the intrusion of random testing when there is no evidence of workplace problems.
USW District 3 Director Stephen Hunt lauded the decision as a “significant victory for not only Steelworkers, but all workers.”
“The safety of workers is paramount and we fight for it every day,” says Hunt. “Random testing is a distraction that invades privacy and does nothing to keep workers and communities safe.”18
#SWPrEP: Policy Outcomes
On November 27, 2017, the Canadian Medical Association Journal published “The Canadian Guidelines on HIV Pre-exposure Prophylaxis and Non-Occupational Post Exposure Prophylaxis.”
In Table 1: “Categories of risk that a person has transmissible HIV infection,” substantial risk is assigned to “HIV status unknown, but from a population with high HIV prevalence compared with the general population (e.g., men who have sex with men, people who inject drugs).”
The guidelines go on to say:
“National data on HIV incidence among sex workers and their clients are scarce, perhaps in part because sex work is criminalized in Canada; as such, this guideline should be applied to these individuals based on the presence of other risk factors.”19
In a December 28, 2017 press release, the B.C. Government Ministry of Health announced new free access to PrEP and expanded PEP for people at risk as of January 1, 2018.
“Effective Jan. 1, 2018, British Columbians at high risk of HIV infection will be able to receive pre-exposure prophylaxis (PrEP), a daily oral antiretroviral medication that prevents new HIV infection, at no cost. …People at risk include men and transwomen who have sex with men, people who inject drugs, and people who have sex with individuals living with HIV.”20
No mention of involvement in commercial sex.
PrEP will be made available through the B.C. Centre for Excellence’s HIV Drug Treatment research program, which is funded by the Ministry of Health through the B.C. PharmaCare program. People interested in accessing PrEP should discuss their personal risks with their health-care provider. PrEP is not to be confused with PEP (Post-Exposure Prophylaxis) where anti-retroviral therapy is given immediately after a possible exposure to HIV to prevent becoming infected. The B.C. Ministry of Health is also expanding the existing free PEP program to include coverage for non-occupational exposure.
Conclusions: Sex Workers and HIV Risks
Making the universal claim that “sex workers are more likely to catch HIV” perpetuates the “sex worker as disease vector” stigma. Sex workers are safe sex professionals!
A recently published study (November 2017), shows that HIV risk is associated with poverty not sex work. “Risk factors for HIV infection among female sex workers in Bangui, Central African Republic” (a country with high overall HIV prevalence of 4.9%) recruited 345 women to examine HIV risk factors for six different categories of female sex workers. “Two groups were the ‘official’ professional FSW” working in hotels and night clubs and “four groups of ‘clandestine’ non-professional FSW” including street and market vendors, girls, students and housewives involved in occasional transactional sex. The study concluded:
“Our observations highlight the high level of vulnerability for HIV acquisition of both poor professional and non-professional ‘street vendor’ FSW categories. These categories should be particularly taken into account when designing specific prevention programs for STIs/HIV control purposes.”21
Every community where ever, and whatever circumstances deserves HIV prevention health care that is distinct and tailored to its individual needs. Sex workers are best placed in society to provide hands-on HIV prevention education and demonstration with the very large and invisible portion of the public who are clients.
Give sex workers the respect we deserve as Safe Sex Professionals.
Footnotes
- “Safety Brief: Truvada for pre-exposure prophylaxis to reduce the risk of HIV-1 infection in adults at high risk — recommendations to support the appropriate use.” Health Product Infowatch, July 2016 p.4-5 http://triple- x.org/safety/prep/HCinfowatch-201607.pdf
- “FDA approves first drug for reducing the risk of sexually acquired HIV infection,” News Release, July 16, 2012 https://triple-x.org/safety/prep/FDAprep-20120712.pdf
- “Did Health Canada just approve Truvada as PrEP?,” Xtra!, February 27, 2015 https://www.dailyxtra.com/did-health-canada-just-approve-truvada-as-prep-70309
- “Guidance for the use of Pre-Exposure Prophylaxis (PrEP) for the prevention of HIV acquisition in British Columbia,” B.C. Centre for Excellence in HIV/AIDS research, 2015 https://triple-x.org/safety/prep/bccfe-prep2014.pdf
- “New York State Summary Statement on Pre-Exposure Prophylaxis to Prevent HIV Infection,” New York State Department of Health AIDS Institute and the Centers for Disease Control and Prevention, October 14, 2015 https://triple-x.org/safety/prep/NYCDCprep-20151014.pdf
- Canadian HIV Pre-exposure Prophylaxis and Non-Occupational Post Exposure Prophylaxis DRAFT Guidelines – Executive Summary, May 12, 2016 http://triple-x.org/safety/prep/CanadianPrEPguide-201605.pdf
- Letter to Kevin Pendergraft, Ad Hoc Committee on Canadian Guidelines for HIV PrEP and nPEP c/o CIHR Canadian HIV Trials Network, Re: Canadian Guidelines for HIV PrEP and nPEP Draft Guidelines, May 31, 2016. http://triple-x.org/about/pr/PrEPguideLetter-160531.pdf
- “Sex Worker HIV Risk” Rapid Review #58: July 2012, Ontario HIV Treatment Network https://triple-x.org/safety/prep/OHTNHIVsexwork-2012.pdf
- “Bringing sex workers to the centre of the HIV response,” the Lancet, July 22, 2014 https://triple-x.org/safety/prep/Lancet-HIVandSW-2014.pdf
- “Global epidemiology of HIV among female sex workers: influence of structural determinants,” the Lancet, July 22, 2014 https://triple-x.org/safety/prep/LancetHIVsexwork-140722.pdf
- Baral S, Beyrer C, Muessig K, et al. “Burden of HIV among female sex workers in low-income and middle-income countries: a systematic review and meta-analysis.” Lancet Infect Dis 2012; 12: 538–49. https://triple-x.org/safety/prep/LancetHIVburden-2012.pdf
- “Review in Slides: Female Sex Workers,” AIDS Data Hub for Asia-Pacific, December 2017 http://www.aidsdatahub.org/female-sex-workers-2017-slides
- “Estimated sizes of key populations for HIV and HCV in BC,” Smart Sex Resource, B.C. Centre for Disease Control, April 4, 2017 https://smartsexresource.com/health-providers/blog/201704/estimated-sizes-key-populations-hiv-and-hcv-bc
- Estimation of Key Population Size of People who Use Injection Drugs (PWID), Men who Have Sex with Men (MSM) and Sex Workers (SW) who are At Risk of Acquiring HIV and Hepatitis C in the Five Health Regions of the Province of British Columbia: Final Report, October 5, 2016. Submitted to the B.C. Centre for Disease Control and the Pacific AIDS Network by The Centre for Global Public Health, University of Manitoba. http://www.bccdc.ca/resource-gallery/Documents/Statistics%20and%20Research/Statistics%20and%20Reports/STI/PSE%20Project%20Final%20Report.pdf
- “The fight against HIV/AIDS just made a monumental breakthrough with this vaccine,” Gay Times, September 27, 2017 http://www.gaytimes.co.uk/news/87967/fight-hivaids-just-made-monumental-breakthrough-vaccine/
- “Antibody detection by agglutination–PCR (ADAP) enables early diagnosis of HIV infection by oral fluid analysis,” Proceedings of the National Academy of Sciences, January 22, 2018 http://www.pnas.org/content/early/2018/01/12/1711004115
- “Position Statement: Influenza Control Policy,” B.C. Nurses Union, March 2015 https://www.bcnu.org/AboutBcnu/Documents/position-statement-influenza-control.pdf
- Steelworkers Arbitration Victory Ends Random Drug and Alcohol Testing At Teck’s Elk Valley Unionized Mines, Media Release, January 29, 2018, United Steel Workers https://www.usw.ca/news/media-centre/articles/2018/arbitration-victory-ends-random-drug-alcohol-testing-at-teck-elk-valley
- “The Canadian Guidelines on HIV Pre-exposure Prophylaxis and Non-Occupational Post Exposure Prophylaxis,” Canadian Medical Association Journal, November 27, 2017 http://www.cmaj.ca/content/cmaj/189/47/E1448.full.pdf
- “Preventative medication will protect people at risk of HIV,” BC Gov News, December 28, 2017 https://news.gov.bc.ca/releases/2017HLTH0114-002108
- “Risk factors for HIV infection among female sex workers in Bangui, Central African Republic,” PLOS One, November 6, 2017 https://triple-x.org/safety/prep/PLOS-RiskFSWBangui.pdf